Bayer’s Next Headache: Draft Guidance


A few weeks ago—four weeks to be exact—Dr. D wrote about Bayer’s New Headache and its Essure System. The FDA promised to provide guidance by the end of February and being true to their word, the agency delivered a draft guidance document, Labeling for Permanent Hysteroscopically-Placed Tubal Implants Intended for Sterilization. Please note the draft document is not binding and was released for comment purposes only. For those readers who did not have an opportunity to read Dr. D’s initial article on the Essure System, according to FDA, “over the past several years, the FDA has been examining the growing number of reports of harm with Essure. The adverse events reported associated with the use of the Essure System include persistent pain, perforation of the uterus and/or fallopian tubes, intra-abdominal or pelvic device migration, abnormal or irregular bleeding, and allergy or hypersensitivity reactions. Some women have had surgical procedures to remove the device. In addition, Essure System failure, and, in some cases, incomplete patient follow-up have resulted in unintended pregnancies.” Unfortunately, the doctor is not enamored with the agency’s draft guidance for this problem device. However, the doctor guesses that someone at Bayer must be quite pleased at the lexical (look-it-up) innovations employed during the scripting of the draft guidance.
Brief History of the Essure System
The Essure System’s premarket approval application (PMA) was initially approved by FDA on November 4, 2002 (P020014). The original PMA was submitted by Conceptus, and on June 5, 2013, this company was acquired by Bayer. According to FDA, there were two conditions associated with the initial PMA approval: (a) the gathering of five-year follow up information on the participants in the two premarket clinical trial patient cohorts (Phase 2 Trial and Pivotal Trial), and (b) the ongoing evaluation of bilateral placement rates for newly trained physicians. Since the initial FDA approval of the PMA, there have been multiple supplements with some of the significant issues being addressed, such as:
- A warning (contraindication) for nickel sensitivity
- Information presented that was associated with the five-year follow-up of clinical data (including pregnancies, which are always bad when talking about contraceptive devices)
- Updated patient risks such as post-procedure patient pain and device migration
FDA’s Guidance
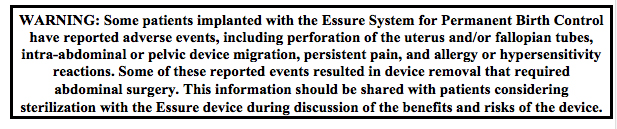
It is Dr. D’s humble opinion that the proposed guidance misses the boat in regards to risk mitigation. The FDA has proposed the placing of a warning label on the device carton (see Figure 1) and a patient checklist consisting of the potential patient acknowledging product risks (through the affixing of patient initials after each question on the checklist). Whatever happened to the good old-fashioned “recall your product until the issues are resolved such as removing the nickel from the product?” Seriously? A warning label? Didn’t Bayer already have a warning label affixed to the product carton? Dr. D would like to suggest that the FDA and Bayer brush up on ISO 14971 and acceptable avenues for mitigating product risk. Yes, the doctor recognizes that the FDA’s recognized consensus version of 14971 is the 2007 version (Recognition Number 5-40). However, using product labeling to mitigate product risk just doesn’t cut it anymore in the device industry. The real solution for reducing product risk “As Far As Possible” (AFAP) is the correcting of flaws in product design. That is Dr. D’s opinion and he is sticking to it!
As for the product labeling, when was the last time a patient asked to see the medical device carton to scan it for warning labels or even better, asked for a copy of the Instructions for Use (IFU) for some light reading prior to a procedure? Can you guess where the product packaging and IFU actually end up prior to or shortly after a procedure? It does not go home with the patient, if you must ask. In fact, answers consisting of the recycling bin (crusher), the trash, or landfill would be more appropriate.
Takeaways
For this week’s guidance there are no takeaways, just a display of Dr. D’s disappointment in the guidance provided. Granted, warning labels and IFUs can provide valuable insight into product utilization and relevant procedural information. However, these days the only people reading the warning labels are the attorneys. It will always be Dr. D’s opinion that the only way to truly mitigate product risk is through product design. Relying on product labeling to address potential product performance issues is not a plan that considers the patient’s best interest. In closing, thank you again for joining Dr. D, and I hope you find value in the guidance provided. Until the next installment of DG, cheers from Dr. D., and best wishes for continued professional success.
References
- Devine, C. (2011). Devine guidance for complying with the FDA’s quality system regulation – 21 CFR, Part 820. Charleston, SC: Amazon.
- Devine, C. (2013). Devine guidance for managing key attributes of a FDA-compliant quality management system – 21 CFR, Part 820 Compliance. Charleston, SC: Amazon.
- FDA.(February 2016).Labeling for Permanent Hysteroscopically-Placed Tubal Implants Intended for Sterilization. Accessed February 29, 2016. Retrieved from http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM488020.pdf
- FDA. (February 2016). Regulatory History. Accessed February 2, 2016. Retrieved from http://www.fda.gov/medicaldevices/productsandmedicalprocedures/implantsandprosthetics/essurepermanentbirthcontrol/ucm452270.htm
- FDA. (February 2016). Essure Permanent Birth Control. Accessed February 2, 2016. Retrieved from http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/EssurePermanentBirthControl/default.htm
Related Articles
-

Problems have persisted with the Essure System. What’s FDA’s next move?
-
If you haven’t made the connection yet, you’re in trouble.
-
Adulterated product and QSR compliance issues create the perfect storm for a warning letter.
-
Put significant effort into the design and development planning phase. It really is the road map for a successful design and development process.
-
Significant changes made to the design or processing of finished medical devices, that are safe and effective in their intended use, require the review and subsequent approval of FDA. This includes changes in the indication for use.
-
Part three of the design verification series discusses in detail the steps that should be taken during testing.
